Focused on the prevention of disability and premature death resulting from stroke, abdominal aortic aneurysm, and peripheral arterial disease.
Cerebrovascular Disease
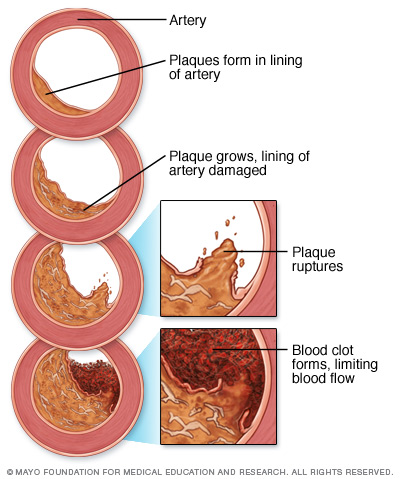
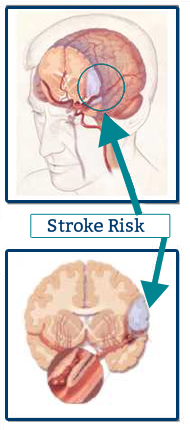 A disease process in which arteries supplying blood to the brain become narrowed or closed off as a result of atherosclerosis. Atherosclerosis or "hardening of the arteries" results from a localized accumulation of lipid-containing (fatty) material, muscle cells, collagen, fibrin, and platelets within or beneath the inner surface of blood vessels. This formation is referred to as plaque and may have many different characteristics. It may appear as a thickening of the blood vessel inner lining, an accumulation of lipids and / or calcific material along the vessel wall, a blood clot (thrombus) formation within the vessel or an ulcerative lesion characterized by deterioration of the plaque surface. It is this plaque formation that causes the blood vessel to become narrowed or closed off, reducing the blood supply to the brain. Plaque formations may also be the source for emboli, plaque that may break loose and travel distally blocking smaller or stenotic vessels. Reduced blood flow to the brain is most often attributed to vessel stenosis, thrombosis, and embolus, all of which may lead to a stroke.
A disease process in which arteries supplying blood to the brain become narrowed or closed off as a result of atherosclerosis. Atherosclerosis or "hardening of the arteries" results from a localized accumulation of lipid-containing (fatty) material, muscle cells, collagen, fibrin, and platelets within or beneath the inner surface of blood vessels. This formation is referred to as plaque and may have many different characteristics. It may appear as a thickening of the blood vessel inner lining, an accumulation of lipids and / or calcific material along the vessel wall, a blood clot (thrombus) formation within the vessel or an ulcerative lesion characterized by deterioration of the plaque surface. It is this plaque formation that causes the blood vessel to become narrowed or closed off, reducing the blood supply to the brain. Plaque formations may also be the source for emboli, plaque that may break loose and travel distally blocking smaller or stenotic vessels. Reduced blood flow to the brain is most often attributed to vessel stenosis, thrombosis, and embolus, all of which may lead to a stroke.
Transient Ischemic Attack (TIA), Reversible Ischemic Neurologic Deficit (RIND), and Vertebrobasilar Insufficiency
Occur when there has been brain tissue damage due to reduced blood flow, which recovers completely with neurological deficits and symptoms resolving over time. Symptoms and neurological deficits may last from a few minutes to a few hours, but may take several days to resolve. This is sometimes referred to as a "mini-stroke".
Cerebrovascular Accident (CVA) Or Stroke
Occurs when there has been irreparable brain tissue damage due to reduced or complete loss of blood flow resulting in permanent neurological deficit.
RECOMMENDATIONS FOR CAROTID DUPLEX SCAN FOLLOW-UP.jpg)
20 - 50% STENOSIS ANNUAL EXAM
50 - 70% STENOSIS EVERY 6 MONTHS
80 - 99% STENOSIS SURGERY USUALLY RECOMMENDED
POST ENDARTERECTOMY
- 6 WEEKS
- 6 MONTHS
- 1 YEAR
- ANNUALLY THEREAFTER
Abdominal Aortic Aneurysm (AAA)
Defined as a 50% increase in the diameter of the aorta or as an aortic diameter > 3.0cm. Normal aortic diameter is 2.0cm (Lederle et al, 1997).
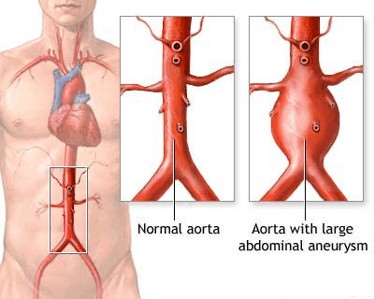 The abdominal aorta is the main artery that supplies blood flow to the organs within the abdomen and pelvis as well as the lower extremities. The aorta can become dilated as a result of atherosclerosis, poor arterial nutrition, congenital defect, infection, trauma or injury. The most common location for arterial aneurysms is the infrarenal abdominal aorta (below the level of the arteries to the kidneys), but they can occur in nearly any artery of the body. Patients with one aneurysm have a higher chance of having a second aneurysm. Other locations for aneurysmal formation are the thoracic aorta, femoral, popliteal, carotid, renal, and splenic arteries.
The abdominal aorta is the main artery that supplies blood flow to the organs within the abdomen and pelvis as well as the lower extremities. The aorta can become dilated as a result of atherosclerosis, poor arterial nutrition, congenital defect, infection, trauma or injury. The most common location for arterial aneurysms is the infrarenal abdominal aorta (below the level of the arteries to the kidneys), but they can occur in nearly any artery of the body. Patients with one aneurysm have a higher chance of having a second aneurysm. Other locations for aneurysmal formation are the thoracic aorta, femoral, popliteal, carotid, renal, and splenic arteries.
The main complications associated with an aneurysm of the abdominal aorta are rupture or peripheral embolization (pieces of thrombus / clot formed at the aneurysm wall break off and travel to the small vessels in the lower limbs blocking blood flow). Because the signs and symptoms associated with an AAA are nonspecific, AAA may be over-diagnosed or under-diagnosed. The clinical presentation of ruptured AAA can be mistaken for other conditions.
AAA may often be found when diagnostic imaging procedures are performed for other reasons or when intentional screening of high-risk individuals is carried out. Once the diagnosis of AAA is made, close follow-up to monitor changes in aneurysm size or surgical repair may be necessary.
FOLLOW-UP ULTRASOUND IMAGING
Recommended at 3 - 6 month intervals after initial diagnosis, with subsequent ultrasound exams every 6 - 12 months for small (<5cm) stable aneurysms
SURGICAL REPAIR may be indicated in the following instances:
- AAA > 5cm in diameter
- > 1cm / year growth
- Symptomatic AAA of any size
- Suspected dissection or rupture
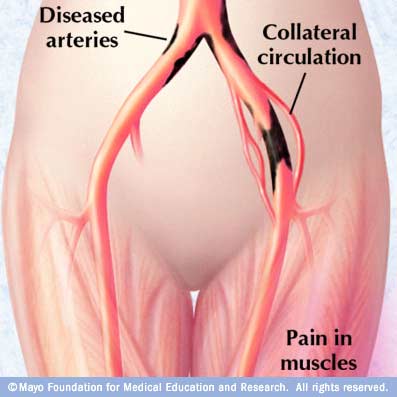
 Peripheral Arterial Disease (PAD)
Peripheral Arterial Disease (PAD)
Resulting from atherosclerosis is one of the most significant health problems affecting the elderly today, and intermittent claudication is its primary symptom.
Intermittent Claudication
A pain or ache in muscle groups of the lower limbs that intensifies during walking and is relieved by rest, results from decreased blood supply or poor circulation to exercising muscles. Although claudication affects millions
of Americans (most of whom are older than 65 years) it is estimated that most patients - an estimated 75% - are undiagnosed.
Physicians estimate that about half their patients don't report their leg pain, either because they don't regard the pain as a medical problem or they view it as an inevitable consequence of the aging process. Reports have shown that the prevalence of intermittent claudication in the younger population, age 30 - 44 years, is greater among men than women. However in the oldest age group, 65 - 74 years, it is almost as high in women as in men.
 Simple, accurate, low cost, noninvasive, testing is available to determine if you are among those with peripheral arterial disease. Testing can be done for the upper and lower extremities, as well as the digits (toes / fingers). Testing is also useful in predicting whether there is sufficient blood flow to heal ulcerations and wounds.
Simple, accurate, low cost, noninvasive, testing is available to determine if you are among those with peripheral arterial disease. Testing can be done for the upper and lower extremities, as well as the digits (toes / fingers). Testing is also useful in predicting whether there is sufficient blood flow to heal ulcerations and wounds.
Vascular Disease Risk Factors
• Cigarette smoking
• Hypertension (blood pressure > 135/85)
• Diabetes (Hgb A1C over 6.3% or FBS over 126)
• Elevated cholesterol and / or triglycerides
• Elevated C-reactive protein
• Obesity (overweight by 20% or more)
• Sedentary life-style (exercise < 3 times per week)
• High stress levels
• Family history
Vascular Disease Signs And SymptomsCerbrovascular diseaseSudden numbness / weakness of the face, arm or leg, especially on one side of the body STROKE IS A MEDICAL EMERGENCY, RECOGNIZE THE WARNING SIGNS. If you experience any of the above signs and symptoms seek immediate medical attention! Abdominal Aortic AneurysmAge > 50 with a history of smoking, hypertension, and coronary or peripheral arterial disease Peripheral Arterial DiseasePain in your legs, thighs or buttocks while walking that worsens with increased activity |